
Amyotrophic lateral sclerosis (ALS) is a progressive disease of the central nervous system. It leads to paralysis that affects speech, swallowing and breathing. So far there is no cure, but appropriate therapy can alleviate the symptoms and increase life expectancy.
- © Getty Images/herraez
Quick Overview: Amyotrophic Lateral Sclerosis (ALS)
Definition: The degenerative disease of the central nervous system leads to progressive destruction of nerve cells in the brain and spinal cord. Since motor nerve cells (motor neurons) are affected, ALS is one of the motor neuron diseases.
Symptoms: After the first muscular failures, there are massive difficulties with swallowing, speaking and breathing and later on paralysis of the entire body musculature.
Course: ALS is incurable and usually leads to death within about two to five years.
Therapy: There are treatment options that can slow down the progression of the disease and significantly improve the quality of life.
Article content at a glance:
Brain: Myths and Surprising Facts

What is ALS?
Amyotrophic lateral sclerosis (ALS) is a progressive disease in which nerve cells die. As a result, there is increasing muscle atrophy and limited mobility.
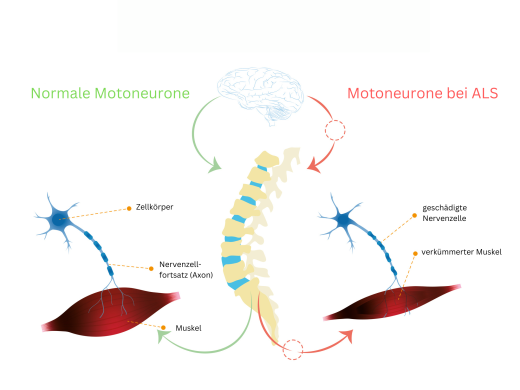
ALS is a disease of the first and second motor neurons. These nerve cells are responsible for the execution of voluntarily controlled movements, i.e. for motor functions. The first (upper) motor neurons originate in the brain and travel through the spinal cord to the vertebral bodies. In the spinal cord, the signals are transmitted to a second (lower) motor neuron, which then continues to the corresponding muscle attachment.
-
© Getty Images/Maria Pilar Martinez Aguerri, Lifeline
special forms:
primary lateral sclerosis: In this special form, only the first motor neuron is damaged. It occurs at a younger age than classic ALS, progresses much more slowly, and has a milder course. British astrophysicist Stephen Hawking was diagnosed with the nervous disorder at the age of 21 and died at the age of 76.
progressive spinal muscular atrophy (PMA): A very rare variant in which only the second motor neuron is affected. The course and symptoms are also somewhat slower and milder.
ALS with frontotemporal dementia (ALS-FTD): Here, the neurons in the frontal lobe of the brain are attacked at an early stage. These people often experience behavioral problems and personality changes.
Frequency of ALS
Although amyotrophic lateral sclerosis is the most common form of motor neuron disease, it is relatively rare. Two out of 100,000 people in Germany fall ill every year. The peak of the disease is around the age of 60. Overall, men are affected slightly more often than women.
In the early stages, symptoms of ALS are unremarkable
The disease begins insidiously and inconspicuously. Those affected usually notice clumsiness as the first sign. You trip or drop something more often than usual.
Possible complaints:
- asymmetric muscle weakness
- low muscle resilience
- general fatigue
- painful muscle spasms
- Speech disorders (dysarthria)
- Swallowing disorders (dysphagia)
However, these symptoms can indicate many different diseases. Nervous disorders such as a herniated disc, myopathy or a stroke (apoplexy) are much more likely to be the triggers.
Stroke: recognize precursors and acute symptoms

Symptoms and complications in advanced stages
The symptoms almost always spread continuously and then lead to the typical full picture of classic ALS: painless paralysis all over the body in combination with spastic (spasmodic) symptoms of various degrees.
Exceptions are the heart muscle, the eye muscles and the sphincter muscles of the bladder and intestines, which are not normally affected in ALS.
In the advanced stage, involuntary muscle twitching often occurs. They are usually not painful. The spasms almost always eventually result in complete paralysis of the skeletal muscles (tetraplegia) and total loss of all motor skills.
Possible symptoms in the course of ALS:
slowed breathing and pauses in breathing
Difficulty sleeping due to nocturnal breathing problems
Fatigue, concentration problems and headaches
Accumulation of secretions in the respiratory tract
Respiratory infections and inflammation of the lungs (pneumonia)
Difficulty swallowing, chewing problems, refusing to eat and weight loss
Spread of paralysis (paresis) with complete loss of muscle mobility
muscle wasting (muscle atrophy)
involuntary twitching of muscles (fasciculations)
pathological laughing, yawning, or crying when the person doesn’t feel like it
Since it is a motor nerve disease, sensory disturbances are not usually among the symptoms. Cognitive functions are also hardly restricted in classic ALS for a long time. Patients often keep an alert, functioning mind to the end.
Causes of ALS are largely unknown
It is still unclear why ALS develops. Only a few of those affected have a hereditary predisposition.
In over 90 percent of cases, the disease occurs without an identifiable cause. This form is called sporadic ALS.
In about 10 percent of those affected, a familial accumulation can be determined, which speaks for a gene mutation. At least seven different genes can be considered as triggers, usually a combination of several genetic defects is present.
ALS is particularly common on some islands in the western Pacific. It also takes a different course with progressive dementia and Parkinson’s symptoms. This endemic form is known as Western Pacific ALS or ALS PD complex.
Diagnosis by excluding other diseases
If ALS is suspected, doctors have neurological examination methods and imaging procedures at their disposal. Experts only speak of ALS when these examinations have clearly revealed damage to the first and second motor neurons.
First of all, diseases with similar symptoms must be ruled out with certainty. For example, various nervous diseases such as polyneurosis, muscle diseases, autoimmune diseases or a herniated disc come into question.
Possible investigations:
Electromyography (EMG): Measurement of electrical muscle activity
Electroneurography (ENG): measurement of nerve conduction velocity
spinal and cranial MRI: Scans of the brain and spine
CSF diagnostics: Examination of the cerebrospinal fluid
Blood Tests: ESR, CRP, CBC, GOT, GPT, TSH, Vitamin B12, Electrophoresis, CK, Creatinine, Electrolytes, Glucose
Laboratory values: exclusion of autoimmune diseases or bacterial infections such as Lyme disease or syphilis (lues)
Genetic diagnostics: if there is a suspicion of a family predisposition
CSF and blood serum can be examined for neurofilaments (NFL) for differential diagnosis and assessment of the prognosis. These proteins form the scaffolding of nerve cells. When neurons die, as in ALS, NFL is released and can be used as a biomarker.
Blood count: important values and what they mean

How can ALS be treated?
So far there is no therapy that can cure ALS. Therefore, treatment focuses on relieving symptoms and improving quality of life. It is advisable to seek advice from a clinic specializing in ALS.
Riluzole is an active ingredient that can slow down the progression of nerve lesions. The drug slows the disease process and increases average survival time by about three to four months. Possible side effects of riluzole are nausea, vomiting, diarrhea, tiredness and increased liver values.
Various active substances are available for the symptomatic therapy of the complaints:
- Antibiotics for pneumonia
- Painkillers for muscle pain
- Magnesium and quinine sulfate against muscle cramps
- expectorant drugs such as N-acetylcysteine
- Anticholinergic drugs to inhibit salivation, possibly also injections of botulinum toxin (Botox) into the salivary glands
General measures for therapy
Physiotherapy is promising in the early stages to maintain mobility. In addition, occupational therapy and speech and swallowing problems can be very helpful. If mobility is restricted, aids such as walking sticks, walkers and wheelchairs are used in order to maintain the patients’ independence for as long as possible.
Advanced stage therapy
In the advanced state of the disease, life-sustaining measures such as ventilation and artificial nutrition are in the foreground:
Treat breathing problems: First, breathing exercises, tapping massages and expectorant measures can be taken. Ventilation with a mobile ventilator and a breathing mask may later be necessary. If the respiratory muscles are so weak that the lungs are no longer adequately ventilated, mechanical ventilation must be used.
gastric tube: Difficulty swallowing often leads to malnutrition and dehydration. High-calorie, liquid food can be fed through a gastric tube.
voice computer: They facilitate communication with speech disorders. Alternatively, a picture board can be used that shows letters, numbers or important care terms (e.g. pain intensity or needs such as hunger and thirst).
Psychotherapy: Due to the severity of the disease, anxiety and depression occur in the early stages. It is important that those affected and their relatives receive professional psychotherapeutic support. In some cases, psychological symptoms can also be improved by medication such as antidepressants.
Course, prognosis and life expectancy in ALS
With classic ALS, life expectancy is not particularly high. ALS is still considered incurable and most sufferers die within two to five years. Only about 10 percent live longer than five years, about five percent longer than ten years. However, the life expectancy is better for the various special forms.
Despite the serious illness and the overall poor prognosis, a relatively good quality of life is often possible even in the advanced course of the disease.
Cause of death in ALS
Ultimately, failure of the respiratory muscles leads to death in most patients. Experts speak of increasing respiratory insufficiency. The weakening of the respiratory muscles does not primarily lead to a lack of oxygen, but to an excess of carbon dioxide, which makes those affected increasingly tired. In this respect, ALS usually leads to slower falling asleep.
Psychotherapy: What forms of therapy are there?
